

Rheumatic heart disease remains a long term health burden in Western Australia yet is largely preventable, particularly amongst Indigenous Australians.
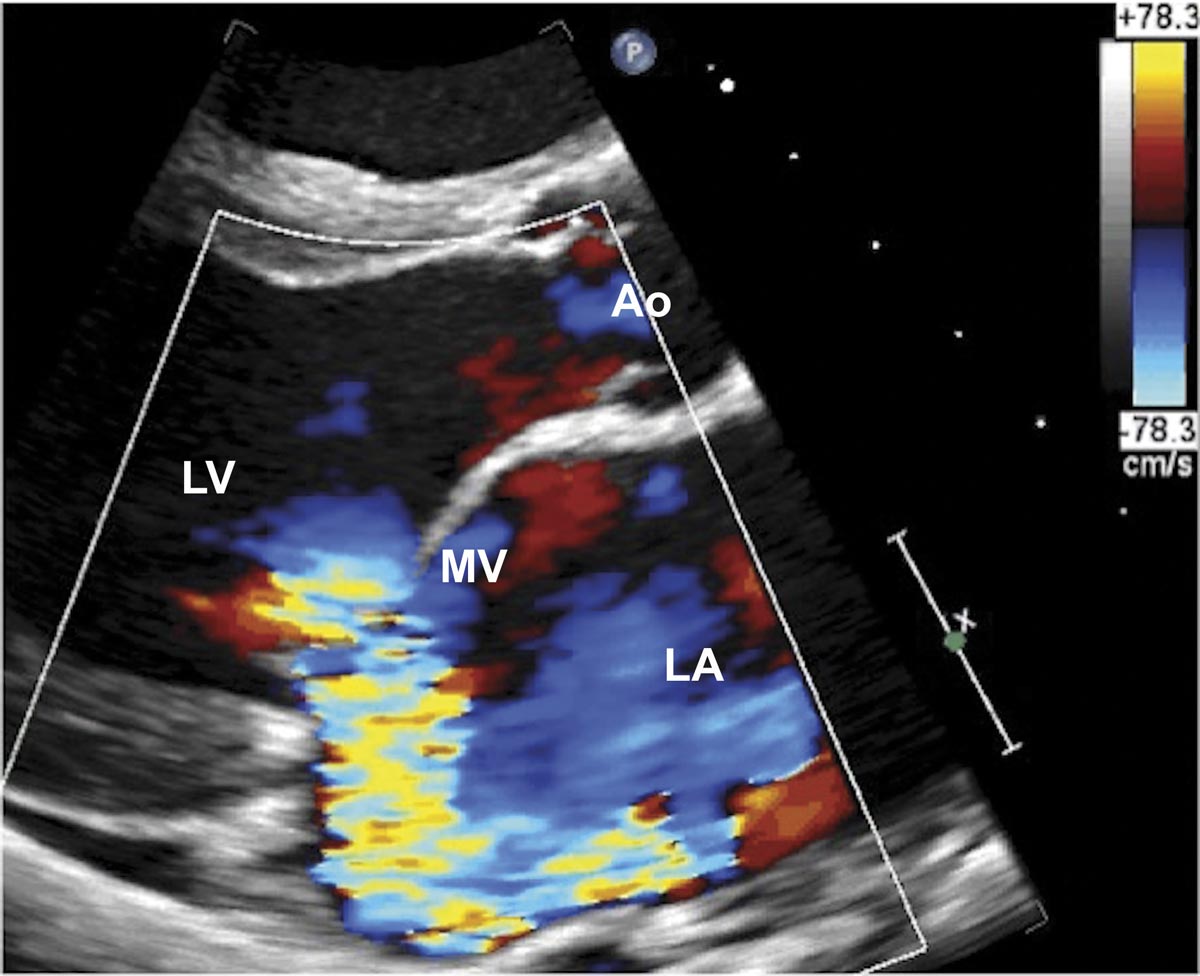
Acute rheumatic fever (ARF) results from a group A Streptococcus (GAS) pharyngeal infection leading to immune-mediated tissue injury. About 60-65% of patients with initial or recurrent ARF episodes develop rheumatic heart disease (RHD). This causes significant morbidity and mortality from serious cardiac sequelae (e.g. heart failure, endocarditis, arrhythmias, stroke). Mitral and aortic valves are most commonly affected, and significant valve disease may require valve repair or replacement.
RHD is almost entirely preventable yet remains a major public health challenge in developing countries and poor, disadvantaged communities. The rates of ARF and RHD among Indigenous Australians are one of the highest worldwide – in WA the prevalence of RHD for Indigenous Australians is 3.9 per 1000 and they are seven times more likely to be hospitalised and five times more likely to die from RHD than non-Indigenous Australians.
The Jones criteria for ARF diagnosis were modified in 2012 to increase the sensitivity of diagnosis amongst Indigenous Australians. The main changes include adding monoarthritis as a minor manifestation and identifying ARF recurrence using one major plus one minor criteria in high-risk groups. If there is a high clinical suspicion but symptoms/signs do not fulfil criteria, these patients may be managed as possible/probable ARF.
The World Heart Federation has developed echocardiographic criteria for RHD diagnosis and defines definite or borderline RHD groups based on mitral and aortic valve pathologic features, Doppler, and mitral valve gradients.
The only proven strategy to prevent recurrent ARF and RHD progression is intramuscular benzathine penicillin G (or erythromycin if allergic to penicillin) every 3-4 weeks, for a minimum of 10 years or until 21 years (whichever is longest).
The greatest challenge to secondary prophylaxis is adherence, thus culturally sensitive education and Indigenous community support are integral to the success of prevention. In addition, initiatives to improve housing, healthcare access and resource provision to Indigenous communities are paramount. Primary prevention through treating GAS pharyngitis with antibiotics is an unsustainable long-term strategy, and considerable research is invested into developing a GAS vaccine.
The advent of affordable portable handheld echocardiography (HAND) devices has gained research interest in population-based screening and early detection of RHD. Whilst not yet adopted in clinical practice, there is ongoing research into the feasibility of HAND in high-disease burden areas as a screening, triage and surveillance tool for RHD. This has significant potential cost-economic benefits and is a step towards improving the health outcomes of Indigenous Australians.
Key Points
- Acute rheumatic fever and rheumatic heart disease remain significant health issues in Indigenous Australians.
- The disparity in ARF/RHD burden between Indigenous and non-Indigenous Australians is large.
- Handheld echocardiography devices may have a role as a screening, triage and surveillance tool for RHD.
Author competing interests: nil relevant disclosures. Questions? Contact the editor.
Disclaimer: Please note, this website is not a substitute for independent professional advice. Nothing contained in this website is intended to be used as medical advice and it is not intended to be used to diagnose, treat, cure or prevent any disease, nor should it be used for therapeutic purposes or as a substitute for your own health professional’s advice. Opinions expressed at this website do not necessarily reflect those of Medical Forum magazine. Medical Forum makes no warranties about any of the content of this website, nor any representations or undertakings about any content of any other website referred to, or accessible, through this website.