

What if someone with atrial fibrillation (AF) doesn’t tolerate warfarin or Novel Oral Anticoagulants (NOACs)? Some alternative treatments still reduce the risk of ischemic stroke in these patients and have better outcomes than doing nothing.
Treating the risk
Atrial fibrillation is a common disease of ageing, affecting 2% of the population (or >10% in people over 80 years).
The loss of atrial contractility in patients with AF results in sluggish flow in the left atrium and left atrial appendage (LAA) which is a remnant outpouching arising from the left atrium. As a result, the risk of clot formation and subsequent stroke (or embolism to other organs) is increased.

Clot formation in AF patients tend to occur in the LAA (up to 90%).
The risk of stroke in AF patients tends to increase with age but other risk factors such as congestive cardiac failure, hypertension, diabetes, female sex and existing vascular disease also contribute to this risk (CHA2DS2-VASc score). Currently, it is recommended that anyone with AF over the age of 65 or has at least one of the mentioned risk factors should be considered for oral anticoagulation.
The most serious side-effect from oral anticoagulation is intracranial or gastro-intestinal bleeding. Patients with significant high risk of bleeding (falls risk or underlying haematological disease) and AF, present a problem.
New technique
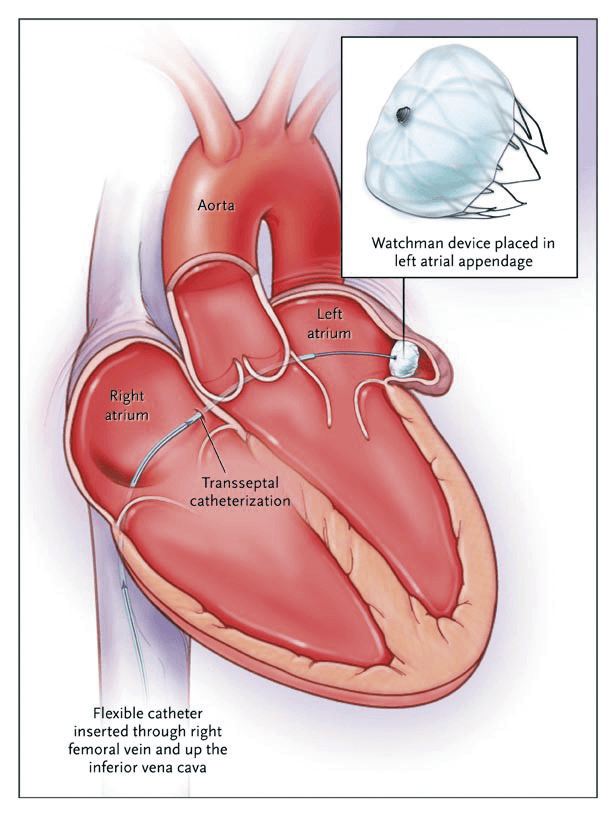
Technology recently approved for Medicare re-imbursement addresses this common clinical scenario. Left atrial appendage occlusion excludes the LAA from the circulation. It is a procedure that plugs the LAA with a special device (the Watchman device or Amulet device) delivered via the femoral vein. Performed under general anaesthesia with transesophageal echo and fluoroscopic guidance in a cathlab, the procedure takes approximately 30 minutes with patients discharged the following day and carries minimal risk (<2% major bleeding, pericardial effusion, stroke). Patients can come off oral anticoagulation long-term after the procedure.
 The safety and efficacy of the procedure was validated with the PROTECT-AF trial1 which randomised 707 patients with AF to receiving long-term oral anticoagulation (warfarin) versus left atrial appendage occlusion (Watchman device). The study found similar rates of ischemic stroke in both groups (1.3% vs 1.1%) but significantly less stroke (of any cause), systemic embolism, and cardiovascular death in the left atrial appendage occlusion cohort at 3.8 years (1.5% absolute reduction). Antithrombotic treatment was given for at least six months after device implantation.
The safety and efficacy of the procedure was validated with the PROTECT-AF trial1 which randomised 707 patients with AF to receiving long-term oral anticoagulation (warfarin) versus left atrial appendage occlusion (Watchman device). The study found similar rates of ischemic stroke in both groups (1.3% vs 1.1%) but significantly less stroke (of any cause), systemic embolism, and cardiovascular death in the left atrial appendage occlusion cohort at 3.8 years (1.5% absolute reduction). Antithrombotic treatment was given for at least six months after device implantation.
Currently, left atrial appendage occlusion is indicated in patients with AF who cannot take oral anticoagulation due to significant bleeding or have an underlying haematological condition that precludes them from taking long-term anticoagulation.
Reference:
- Reddy VY, Sievert H, Halperin J, et al. Percutaneous Left Atrial Appendage Closure vs Warfarin for Atrial Fibrillation: A Randomized Clinical Trial. 2014;312(19):1988–1998. doi:10.1001/jama.2014.15192
Questions? Contact the editor.
Author competing interests: nil relevant disclosures.
Disclaimer: Please note, this website is not a substitute for independent professional advice. Nothing contained in this website is intended to be used as medical advice and it is not intended to be used to diagnose, treat, cure or prevent any disease, nor should it be used for therapeutic purposes or as a substitute for your own health professional’s advice. Opinions expressed at this website do not necessarily reflect those of Medical Forum magazine. Medical Forum makes no warranties about any of the content of this website, nor any representations or undertakings about any content of any other website referred to, or accessible, through this website.