


ED: CMR can be difficult to assess due to shortages of adequately trained specialists and lack of funding.. Nonetheless, CMR is pivotal in the evaluation of cardiomyopathies.
Cardiac MRI (CMR) can be invaluable where the mechanism of cardiac injury is uncertain, with contrast-enhanced imaging providing a ‘virtual histology’ of the myocardium. One such setting is Myocardial Infarction with Non-Obstructed Coronary Arteries (MINOCA), which occurs in 5-10% of angiograms undertaken for acute coronary syndromes.
Case Report
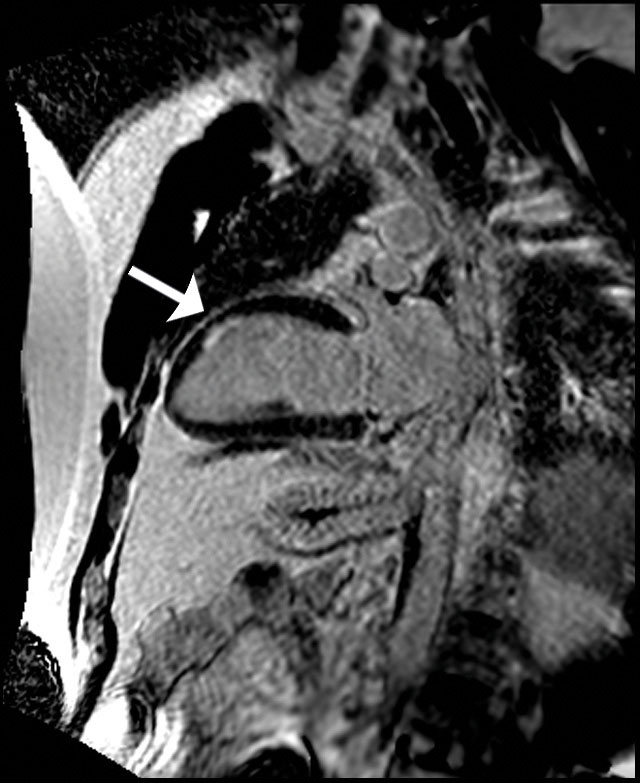
A 41-year-old hypertensive male presented with gripping chest pain after emotional stress. He reported non-specific malaise over the preceding 3 days with a cough. Inflammatory markers were modestly elevated, and Troponin I rose from normal to 150ng/L, with minor anterolateral T wave inversion on ECG. Echocardiography was reported as normal, and angiography documented only mild irregularities. A working diagnosis of myocarditis was made and colchicine was commenced, but dual antiplatelets were also continued due to diagnostic uncertainty. CMR demonstrated a anterior regional wall motion abnormality (not appreciable on echo) with oedema and infarction (figure 1), confirming a conventional ‘heart attack’ rather than myocarditis. Colchicine was discontinued, secondary prevention for acute coronary syndrome was intensified, and further investigations to rule out an embolic aetiology are being sought.
Discussion
MINOCA is a diagnostic conundrum because several diseases can masquerade as a heart attack, including myocarditis, cardiomyopathies, coronary spasm and others. However, 20-40% do represent a true (atherosclerotic) coronary event with spontaneous recanalisation or non-appreciable culprit, thus dual antiplatelet therapy often continues to be prescribed. By extension, this exposes the remaining 60-80% unnecessarily to bleeding risks.
CMR is the gold-standard non-invasive modality for quantifying cardiac volumes and ejection fraction. However, the unique ability of CMR to evaluate cardiac scar is particularly informative, determining not just the presence of abnormality but also the mechanism (infarction, inflammation or infiltration). In a large registry of over 600 individuals, an incremental value of CMR for clinical decision-making in MINOCA was observed in over 80% of cases.(1) The European Society of Cardiology Working Group position paper on MINOCA advocates “cardiac magnetic resonance imaging is the key diagnostic tool to be employed in MINOCA patients.” (2)

Fig 1: Delayed contrast-enhanced imaging with (a) 2-chamber view and (b) short-axis view showing partial-thickness focal sub-endocardial infarction in the mid anterior wall.
Further reading:
- Rajwani A et al. The incremental impact of cardiac MRI on clinical decision-making. Br J Radiol, 2016; 89
- Agewall S et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J, 2017; 38:143-153
Images courtesy of Western Radiology.
Questions? Contact the editor.
Author competing interests: nil relevant disclosures.
Disclaimer: Please note, this website is not a substitute for independent professional advice. Nothing contained in this website is intended to be used as medical advice and it is not intended to be used to diagnose, treat, cure or prevent any disease, nor should it be used for therapeutic purposes or as a substitute for your own health professional’s advice. Opinions expressed at this website do not necessarily reflect those of Medical Forum magazine. Medical Forum makes no warranties about any of the content of this website, nor any representations or undertakings about any content of any other website referred to, or accessible, through this website.