

By Dr Edmund Lee, Interventional Cardiologist, Murdoch
Doctors may feel somewhat bewildered at the back-and-forth of hypertension treatment recommendations over recent years. Are lower goals really better, and how low is too low?

The Joint National Committee (JNC) 7 released in 2003, advised a treatment threshold of 140/90 mm Hg for most adults but included a lower target of 130/80 mm Hg for patients with diabetes or chronic kidney disease. The lower targets were based on observational studies and expert consensus that treating to these would improve cardiovascular outcomes.
The JNC 8 guideline took a different approach by relying primarily on evidence from randomised controlled trials. They only found strong evidence for treating to a BP of 150/90 mm Hg in adults aged 60 years or older and eliminated the lower targets for patients with diabetes and chronic kidney disease, making the goal 140/90 mm Hg for most people.
The SPRINT trial was a study of 9361 participants with systolic blood pressure (SBP) ≥130mmHg with ‘high-risk’ hypertension randomised to either a lower more intensive goal of treatment as <120 mm Hg SBP compared with a goal of less than 140 mm Hg systolic.
The primary outcome here was a combined cardiovascular outcome that included myocardial infarction, stroke, heart failure, or cardiovascular death. The trial was stopped after three years (intended for five years) due to the strongly positive result. The primary endpoint occurred in 1.65%/year in the intensively treated arm (average of 121 systolic) versus 2.19%/year in the standard group (average of 136mmHg systolic), a 25% relative risk reduction. There was also a 27% reduction in all-cause mortality.
However, 4.7% of the intensively treated arm developed symptomatic hypotension, abnormal electrolytes, acute kidney injury or syncope versus 2.5% in the standard arm. Falls with injury were not increased.
Latest guidelines
The new US guidelines, based mostly on the SPRINT result, have made a number of changes. The biggest change would be the new targets for treatment.
Older adults have the same treatment target as younger patients, and drug therapy is recommended for all older adults (age >65 years) with an average systolic pressure of 130 mm Hg or greater.
The guidelines also stress the importance of average BP measurements taken over several visits, as well as out-of-office measurements (see tables 1 and 2).
Table 1: Categories of BP in adults
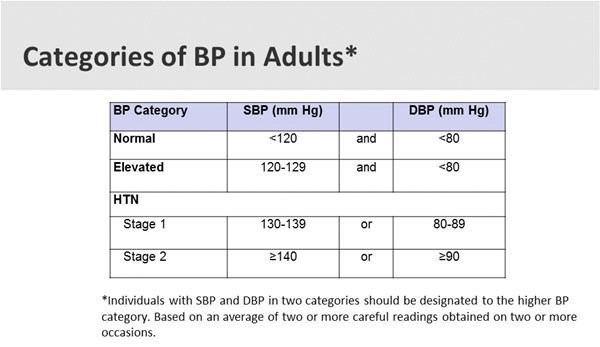
Individuals with SBP and DBP in two categories should be designated to the higher BP category. Based on an average of two or more careful readings obtained on two or more occasions.
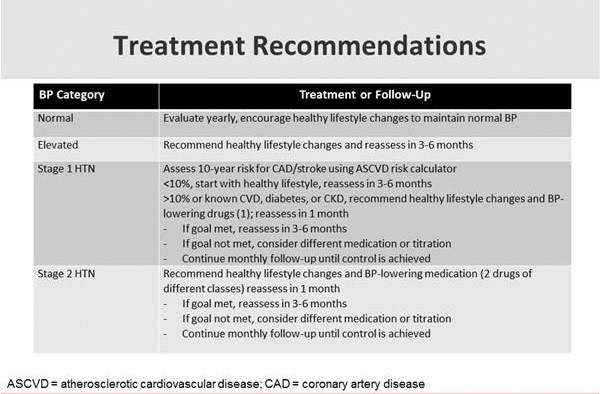
Table 2: Treatment Recommendations
Whilst the change in the US hypertension guidelines is likely to be debated throughout 2018, it may increase hypertension awareness, encourage lifestyle modification and focus antihypertensive medication initiation and intensification in adults with high CVD risk.
Guidelines are just that. They are a demarcation of where we should aim but results vary patient to patient. We don’t necessarily need to push the BP down in older, frailer patients, particularly if there are anticipated side effects such as pre-syncope or the risk of falling.
Key Points
- Hypertension guidelines continue to change based on emerging evidence
- New American (ACC/AHA) guidelines now consider stage I HTN between 130-139/80-89
- Home BP measurements are crucial for diagnosis along with a 24 hour BP measurement as the gold standard test
- Treatment targets should be individualised with potential benefits in achieving lower targets at the expense of side-effects to treatment.
Disclaimer: Please note, this website is not a substitute for independent professional advice. Nothing contained in this website is intended to be used as medical advice and it is not intended to be used to diagnose, treat, cure or prevent any disease, nor should it be used for therapeutic purposes or as a substitute for your own health professional’s advice. Opinions expressed at this website do not necessarily reflect those of Medical Forum magazine. Medical Forum makes no warranties about any of the content of this website, nor any representations or undertakings about any content of any other website referred to, or accessible, through this website.