

ED: Fears about fractures include leaving something too long (for whatever reason) or over-reacting – these practical notes will help those fears.

This article discusses two hand injuries that can be missed and two common hand injuries for which referral directly to a hand therapist may be warranted.
Scaphoid fractures
Many practitioners are concerned about scaphoid fractures but they are relatively simple to diagnose or exclude given a systematic approach.
If you suspect a patient has a scaphoid fracture your first investigation is usually a plain scaphoid radiograph. However, a portion of patients have normal radiographs, so if you still suspect a scaphoid fracture, splint with a forearm-based wrist backslab or splint (there is no requirement to include the thumb in the splint) and organise either a CT (confirms 99% of scaphoid fractures) or an MRI (confirms 100% of scaphoid fractures and can also diagnose soft tissue injuries in the vicinity).
If the CT or MRI is normal you can manage the patient according to their clinical symptoms but if the patient’s recovery is slower than expected it would be worth asking a hand surgeon for their opinion. Any fracture revealed on imaging is managed accordingly.
Jersey finger
Sudden resisted finger flexion can result in an avulsed flexor profundus tendon causing no active flexion of the distal interphalangeal joint but active flexion of the proximal interphalangeal joint usually persists.
A high proportion of these patients present late, which significantly compromises treatment outcome. They should be referred urgently to a hand surgeon.
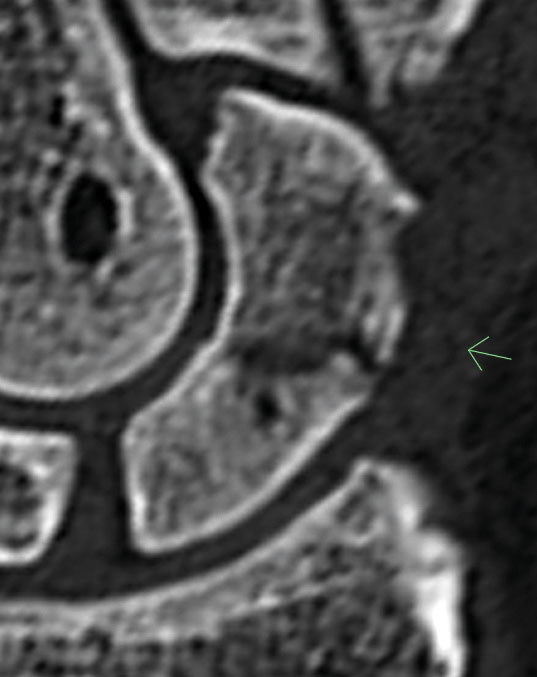
Proximal interphalangeal joint sprain / volar plate injury
Sprains to finger proximal interphalangeal joints are common. Patients will present to you with a stiff and uncomfortable joint which has a fusiform swelling often after a forced extension or staving type injury. X-rays sometime demonstrate a small avulsion fracture at the attachment of the volar plate which is effectively a ligament sprain with a flake of bone attached; this does not represent a problem unless the fragment is large or the joint is subluxed (as in the x-ray beneath).
These injuries are best treated by the hand therapists with initial protection of the finger and subsequent exercises to prevent or treat a late fixed flexion contracture which common occurs without treatment.

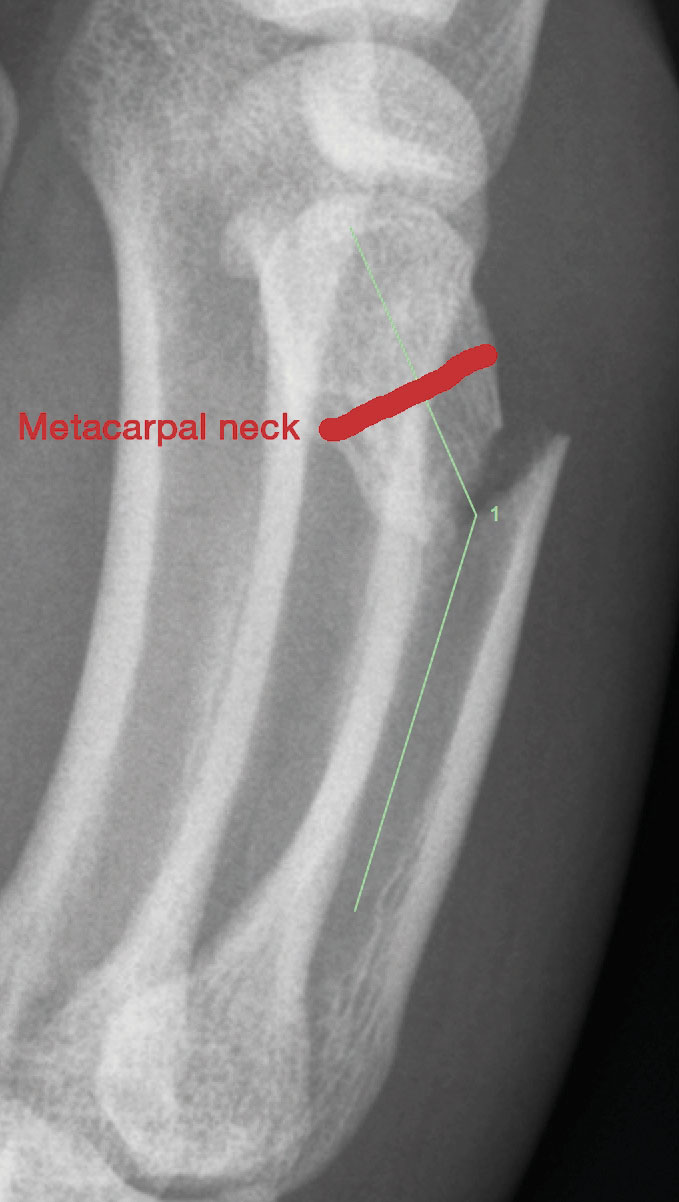
Boxer’s fracture
Little finger metacarpal neck fractures are common and frequently angulate although it is very uncommon for the finger to be rotated. As long as the angulation is under 45 degrees a “less is more” approach is best. Let patients know the end result of non-operative treatment is excellent but that there will be a long-term prominence at the fracture site and their knuckle will be somewhat less prominent compared to pre-injury.
I normally ‘neighbour strap’ two adjoining digits for up to four weeks, allow use of the hand in that time within the limits of comfort.
The hand therapists can provide a Lycra neighbour sleeve, which is more convenient than tape, and if at risk of banging the hand a thermoplastic splint can be used for when the hand requires protection.
However, fractures that are proximal to the neck (see X-ray) fair less well and are best referred to a hand surgeon.
Many hand therapy practises have a close working relationship with a hand surgeon and will discuss with the surgeon if they are concerned surgery should be contemplated.
References available on request.
Questions? Contact the editor.
Author competing interests: nil relevant disclosures.
Disclaimer: Please note, this website is not a substitute for independent professional advice. Nothing contained in this website is intended to be used as medical advice and it is not intended to be used to diagnose, treat, cure or prevent any disease, nor should it be used for therapeutic purposes or as a substitute for your own health professional’s advice. Opinions expressed at this website do not necessarily reflect those of Medical Forum magazine. Medical Forum makes no warranties about any of the content of this website, nor any representations or undertakings about any content of any other website referred to, or accessible, through this website.